Covid-19, how much testing do we need?
Posted on April 6th, 2020
By Chandre Dharmawardana.
A number of distinguished medical professionals led by Dr. Ruvaiz Haniffa , Head, Dept. of Family Medicine, University of Colombo, published an appeal (see the Island , 1st April, Daily Mirror and other newspapers) emphasizing the Need for rapid expansion in testing for COVID-19 in Sri Lanka”.
While creating a data base is essential for constructing epidemiological models, another very effective approach uses information-based intervention. Detectives examining social media or gossip learn about Covid-19 contacts, religious gatherings etc., and aggressively follow every lead. Sri Lanka is currently in stage 3A (WHO classification) where clusters are being identified. To avoid deteriorating to stage 3B, authorities have to trace contacts and isolate cases. This is an intelligence-driven attacking approach” (IDAA). The military in Sri Lanka was thus able to identify over 20,000 people and enforce self-quarantining. Direct sampling would not have found these people, or if found, it would be too late.
So we need BOTH the IDAA and direct TESTING of optimally selected samples.
Even people who seem perfectly healthy may be carries of the virus. Testing suspected cases” may not be enough. But no country can test even a significant fraction of the population? But what is that significant fraction? How can we get away with testing even smaller fractions? How do we sample populations?
Test kits for the new virus are in short supply and now reserved for priority cases. Leading companies are scrambling to provide test kits to countries buckling under the virus. There are also cheap wonder test kits” that quick-buck inventors and alternative-medicine Gurus have put out, claiming fast test results. These should be avoided and only kits using proven methods must be used.
According to Health Canada guide lines, a person with a confirmed virus infection” must have positive nucleic acid amplification tests on at least two specific genome targets or a single positive target with nucleic acid sequencing.
Many Western governments (e.g., France) had comprehensive plans for dealing with Pandemics, put in place after the SAARs epidemic. But the rise of neo-liberals and Human-Rights lobbies with their belief in minimal government intervention and devolution (e.g., in Spain) led to the disbanding of all such programs, leaving matters to the private sector” and to local authorities”. USA is still in that mode and lagging behind in fighting Covid-19. Today, many governments are scrambling to re-assemble those safety nets at great cost.
The article by Dr. Haniffa and his learned colleagues suggests the use of existing laboratories in the country to do the testing. Even if we had 25 such labs, and even if each lab did several hundred tests a day, it is clear that even if test kits are available, the time delay in getting useful answers, coordinating timing and data processing a huge number of samples reliably under emergency conditions is impossible. We need good data in real time. A further six months delay for peer review can be avoided if the program is under medical and scientific experts.
So, testing boils down to the crucial question of what is the smallest sample needed to get at a reliable answer”? The medical professionals had not addressed this most crucial question, but their involvement is needed. Otherwise we can only address the basic statistical question of how big a sample should be, without additional wisdom.
Ramanayake’s Audio files.
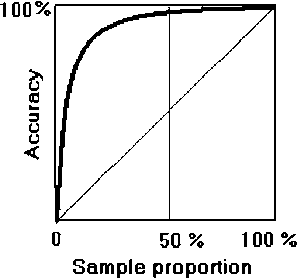
Take a simpler problem. For instance, actor turned MP Ramanayake’s now notorious telephone recordings run into, say 10,000 audio files. It takes too long to review ALL the tapes. What is the minimum number (sample size) of files that we should listen to, to have a very good chance of picking up the most juicy one? Elementary mathematics shows that the sample should be a fraction 1/e of the total, where e” is the number 2.7182 which is the base of Napier’s system of natural logarithms. So, it is probably enough to listen to approximately 10,000 divided by 2.7, i.e., about 3704 audio files to pick up the most interesting one! As the attached graph shows, increasing the sample size even to 50% does not strongly increase the chances of catching the incriminating case significantly.
The same sampling technique can be used if you have to select the best candidate from 1000 applicants to a job. Your best candidate is most likely to be within the first 370 that you interview!
The audio tapes, or candidates for a prescribed job, presumably all form a set of similar objects or individuals. But human populations are not uniform. Even the individuals in the population of each district are still too dis-similar to form a statistically uniform sample”. It is here that judicious planning is needed. Judging that the Covid-19 is most likely to be found in urban populations than in rural populations (say), one may take samples from each city population in a given district. One doesn’t even have to take a census of each city to know their proportions – they follow a mathematical law known as Zipf’s law. In any case, once the uniform demographic to be tested” (having a normal distribution) is identified, one can use the inverse of Napier’s number and so take about 37% of each demographic to make the test samples for each district.
Of course, a good team of statisticians can work out a better statistical models to minimize the sample size, improve the gathering of data and deal with non-normal, multi-modal and other distributions. The data provides an empirical basis for constructing a trustworthy epidemiological model for Covid-19 affecting the country. However, one really needs a time dependent model taking account of the amount of virus (viral load ) absorbed by the patient during the process of infection. The interaction between the virus and the immune system is a race in time. If you get a large dose, you get higher viremia, more dissemination, higher infection, and worse disease.
So, the suggestions by the health professionals must be taken seriously, but using a good sampling scheme rapidly deployed to make the testing affordable and meaningful. This will also be an important research contribution to the epidemiology of the disease. No country should rely on the Covid-19 growth curves of other countries. For instance, the rate of growth of Covid-19 in a country with a large demographic of young people will be quite different from that of an European country with a large demographic of old over-fed people. Furthermore, once a patient is identified as having the virus, there is still no clear way of predicting if the disease will become acute. The British government under Mr. Boris Johnson used a limited epidemiological model constructed by Imperial College, London, and is said to have paid the price in money and lives on being misled on how Covid-19 will develop in the UK.
Sri Lanka should also attempt making its own vaccines. Time-tested techniques for making SARS-CoV-2 vaccines are by inactivating whole virus particles with formaldehyde and adding a booster like alum, and doing clinical trials.
All this can be derailed by a politically powerful Natha Deiyyo devotee” who may come forward with a quick revelation of what the status of the epidemic is, after claiming that Western Science is a Patta Pal Boru” fabrication, as happened with the investigation of the Chronic Kidney Disease Endemic affecting the North Central Province of Sri Lanka. Similarly, die-hard Muslim groups have already risen asking for Mulsim burials (bathing the corpse etc.), showing the ever persistent power of faith over reason.
By Chandre Dharmawardana.