Eradicating CKDu From Sri Lanka is Straightforward—What is Preventing it?
Posted on December 8th, 2023
by Drs. Sunil J. Wimalawansa (Prof. of Medicine)and Chandra B. Dissanayake (Prof. of Geology)

Since identifying chronic kidney disease of unknown etiology (CKDu) in Sri Lanka in the mid-1990s, little progress has been made in aetiology and prevention. Despite the numerous hypotheses and conjectures—with more than 35—none have been thoroughly studied or substantiated as the definitive cause of CKDu.
The development of CKDu necessitates simultaneous exposure to various factors and conditions over an extended period. Hence, it is also called chronic kidney disease of multifactorial origin (CKDmfo). A recent newspaper article suggested that Chinese researchers re-confirmed the lack of association of agrochemicals, heavy metals, or arsenic (common postulated factors) with CKDu, consistent with our and other scientists’ publications over 15 years.
Comparatively, on a per-hectare basis of arable land, New Zealand and numerous other countries employ more than ten-fold the amount of agrochemicals and fertilisers containing heavy metals. Similarly, in Sri Lanka, in hilly country like Nuwara Eliya, and wet zones, farmers extensively utilize inorganic fertilisers, especially phosphates and pesticides—significantly more than in the dry zones. Surprisingly, there is little to no reported incidence of CKDu in these regions.
Research studies on hypothesis-driven causation are needed
The lack of conclusive evidence on CKDu stems from inadequately designed studies that fail to assess causes and test specific hypotheses. No CKDu study has rigorously applied Hill’s criteria for disease causation to distinguish casual association from causation. To address CKDu causes effectively, detailed empirical studies, not just descriptive ones, are essential. [For more details, refer to Hill, A.B., 1965, The Environment and Disease: Association or Causation?”]
(https://www.ncbi.nlm.nih.gov/pubmed/14283879].
No credible scientific evidence supports the role of any of the mentioned postulated factors in contributing to or causing CKDu. Definitive conclusions necessitate well-conducted, unbiased studies with proper design and sufficient statistical power to thoroughly assess or rule out the potential effects of heavy metals, algal toxins, and agrochemicals on CKDu.
Critical causative criteria for establishing a link between a factor and a disease include the Strength of the association, Consistency, Specificity, Temporality, Biological gradient, Plausibility, Coherence, and Empirical data (Experiments). The presence of the majority of these factors is necessary to attribute causation. However, most studies on CKDu are heterogeneous and descriptive, offering limited value. Therefore, conducting meta-analyses using such data is scientifically unsound and inappropriate, as they will likely yield misleading conclusions.
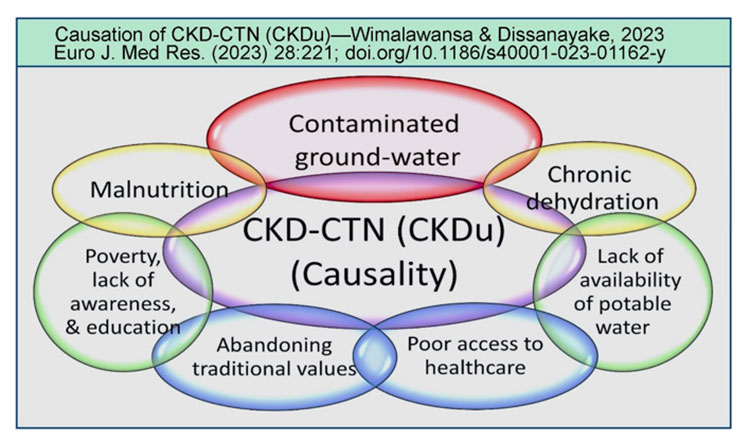
Because CKDu arises from forming nanocrystals and nanotubes in kidney tubules and tissues, a more fitting designation would be CKD of crystal-tubular nephropathy” (CKD-CTN). The accompanying figure illustrates critical factors contributing to the CKD-CTN development (from Wimalwansa & Dissanayake, Euro. J. Med. Res., July 2023: https://rdcu.be/dgagf). (See Figure)
Poorly designed studies generated inconclusive data:
Compartmentalized research and poor study designs consistently fail to address research questions and test hypotheses related to CKDu. This lack of adherence to fundamental scientific principles, along with issues in improper sample collection and data integrity, has resulted in skewed and unreliable conclusions, muddling the progress and analyses of CKDu in the country.
Extrapolating such data to the overall status of CKDu in Sri Lanka and other tropical countries shifts attention away from identifying actual causative factors, proper fund allocation, and implementing essential remedies for CKDu prevention. Biased comments by Chinese scientists, such as ‘aristolochic acid,’ while relevant in rural China, are not pertinent to CKDu (CKD-CTN) in the dry zones of Sri Lanka.
Methodological and conceptual failures:
No conclusive evidence supports agrochemicals (glyphosate) or heavy metals causing CKDu. Claims linking slightly elevated magnesium in drinking water to CKDu lack reliability due to sampling and methodological errors. In contrast, over 750 international research articles establish magnesium as a renal protector” in humans.
Detecting an isolated elevation of magnesium or extremely low levels of glyphosate in inconsistent studies is insufficient to establish even an association, let alone causation. Such findings meet only one of Hill’s Causation criteria. Inferences from random water samples and two rat studies lack reproducibility and conclusiveness. The flawed extrapolation of this data to assert that glyphosate or magnesium causes CKDu has diverted attention and national research funds to unproductive programmes. The crucial factor in drinking water is the calcium to magnesium” ratio, not individual components alone.
Glyphosate or other chemicals used in intervention experiments, equivalent to body weight on a kg basis, are astronomically” high—toxic. Such concentrations do not exist in water or soil under normal conditions. Such concentration exists when an individual ingests concentrated glyphosate. Therefore, conclusions from such experiments are misleading. Any toxicity dependent on the dose and exposure” and real-world scenarios do not match the extreme concentrations used in intervention experiments.
Studies have consistently lacked rigorousness during sample collection, standardized methodology, and the use of controls. They also lack quality control during analyses and testing hypotheses. Methodological errors, such as smaller sample sizes and a lack of control experiments, introduce random- and Type-2 errors into the data. To obtain accurate insights, examining thousands of properly collected water samples across affected regions is crucial, as is comparing them with comparable but non-affected villages within the same region (e.g., subtractive analysis), even within ‘affected’ villages, pockets with good-quality drinking water (e.g., natural springs), thus clusters of unaffected families. Therefore, calling the entire area as CKDu affecting is a misnomer.
The neglect of already published data
Suppose one uses CKD” as a keyword in the following URL: one can pull over a dozen research articles illustrating that CKDu is triggered by natural” causes—hard water (Ca2+), excess phosphate in combination with fluoride” and chronic dehydration.
https://www.researchgate.net/profile/Sunil-Wimalawansa/publications
Peasants experiencing chronic dehydration due to daily exposure to hot climates and nightly alcohol intake, along with drinking water high in Calcium, Carbonate/ Phosphates, and Fluoride ions, etc., create a conducive internal environment” for the formation of calcium phosphate (CaPO4) crystals within renal tissue. Additionally, hard water chelates glyphosate, eliminating its potential toxicity, if any, whereas fluoride has the opposite effect.
Chronic exposure to excess calcium, carbonate/phosphate (and other anions), and fluoride through the ingestion of hard water over a decade is necessary to induce CKD-CTN. Such extended exposure maintains the mentioned higher ionic concentrations in renal tissues. Chronic dehydration leads to consistently concentrated urine, enabling the precipitation of hydroxy- and oxalate-apatite nano-minerals in the kidneys. This process occurs with or without fluoride, but fluoride stabilizes these nano-mineral crystals, forming fluorapatite resistant to degradation, allowing crystals to grow. Fluorapatite nanocrystals are implicated in causing CKD-CTN, causing fatal renal failure. The detailed mechanism is illustrated in the following article: https://www.mdpi.com/2076-3298/7/1/2
The way to prevent and eradicate CKDu:
Consuming potable water and avoiding prolonged dehydration can prevent persistent dehydration-associated CKD-CTN. This concept offers highly cost-effective and straightforward solutions to safeguard peasants, particularly farm laborers. This eliminates silent, deadly disease, without needing expensive medications, interventions, or the construction of dialysis centers and hospitals, which is especially crucial in financially strained circumstances.
Research, including ours, has shown that increasing daily access to clean water significantly reduces CKD-CTN incidence and associated morbidities and premature deaths. Unfortunately, once the disease progresses beyond CKD stage IIIB, the damage becomes irreversible. It leads to hardening and shrinkage of the kidney due to fibrosis—resulting in permanent damage.
The following two published articles provide a detailed methodology and cost-benefit analysis of ways to eradicate CKDu from Sri Lanka:—CKD-CTN.Public health interventions for chronic diseases: cost-benefit modelizations for eradicating chronic kidney disease of multifactorial origin (CKDmfo/ CKDu) from tropical countries. Heliyon 2019;5(10):e02309. DOI: 10.1016/j.heliyon.2019.e02309.And Strategic framework for managing non-communicable diseases: Preventing chronic kidney disease of multifactorial origin (CKDmfo/CKDu) as an Example. Chronic Dis Int 2015;2(2 (1018)):1-9 (https://austinpublishinggroup.com/chronic-diseases/fulltext/chronicdiseases-v2-id1018.php).
The direct approaches outlined in the above articles offer ways to mitigate and eradicate CKDu/CKD-CTN in Sri Lanka and other affected countries. Unfortunately, there has been a lack of political will to address the issue. For some, it has become an unscrupulous business. The mentioned scientific papers provide details on how implementing a multi-pronged approach can prevent CKD-CTN, reduce premature deaths, and minimize the socio-economic impact on affected families. For more information. More information in:
Environmental health and preventive medicine 2014;19(6):375-394. DOI: 10.1007/s12199-014-0395-5 (https://pubmed.ncbi.nlm.nih.gov/25239006/).
Critical elements need to eradicate CKD-CTN from Sri Lanka
It is essential to systematically address peasants’ lifestyles and dietary habits, improve micro-nutrition, protect their renal and general health, and mitigate CKD-CTN. In addition to providing potable water, other interventions are also necessary to overcome this forgotten killer. Adhering to such would save the lives of people in CKD-CTN-affected tropical countries. They consume insufficient water due to the unpleasant taste of naturally contaminated hard water. Just because peasants do not have a voice is not an excuse to neglect them by the politicians and the government.
The key to eradicating CKD-CTN is prevention through education, lifestyle changes, and increased consumption of clean water—not in treating renal disease or expanding dialysis centers, hospitals, or transplantation services. To effectively prevent CKD-CTN, providing safe and affordable clean water in the affected and adjacent regions in the entire dry zone is essential rather than solely emphasizing aggressive treatment of end-stage renal diseases.
Historical evidence indicates that ancient Sri Lankan Kingdoms, like Anuradhapura, Polonnaruwa, Dambadeniys, Sigiriya, and Yapahuwa, were relocated, primarily within the dry zonal regions, now affected by CKD-CTN. The reasons for these relocations, whether protecting from invading armies, severe malarial epidemics, or deaths due to CKD-CTN, remain uncertain. Proposals to move the entire North Central Province (NCP) population elsewhere or replace the topsoil in the region are deemed impractical and absurd.
The current approach will continue to fail
The current strategy of expanding renal clinics, dialysis and transplantation services, coupled with reliance on aid from other countries, is an ineffective approach that falls short of preventing and eradicating” CKD-CTN in Sri Lanka. This method is like holding a tail to tame a tiger. Even if the rates of deaths have somewhat slowed, it is likely because many of the most vulnerable individuals are already deceased. The focus should shift towards protecting the younger generation and families. Unfortunately, CKDu has become a business venture for many, akin to exploitation during the LTTE war.
In addressing CKD-CTN, vision, political will, and prioritization of programs that cost less than a few months of healthcare expenses for maintaining affected individuals and families are lacking. Sri Lanka possesses the necessary technology, know-how, and essential resources to implement a program for eradication without requiring international expertise. However, inherent conflicts of interest hinder the implementation of the right path and impede progress.
Our latest contribution on the subject [Title: Nanocrystal-induced Chronic Tubular-nephropathy in Tropical Countries: Diagnosis, Mitigation, and Eradication] published on July 2023 in a Nature Journal (EJMR)—PDF of the article available from the following links: https://rdcu.be/dgagf