CHRONIC KIDNEY DISEASE AND EELAM Pt 1
Posted on December 10th, 2016
KAMALIKA PIERIS
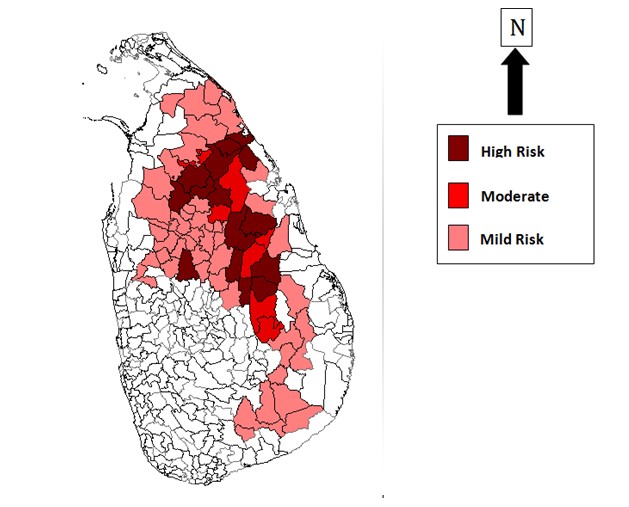
‘Chronic kidney disease of unknown origin’ (CKDu) came to the attention of the medical profession of Sri Lanka in 1991 when the first cases with terminal renal failure started coming in. It was officially reported in the mid 1990s. The reports came mainly from the North Central province. CKDu was first detected in Padaviya. Thereafter, cases were reported from 10 Divisional Secretariat divisions of the NCP, particularly Medawachchiya, Padaviya, Kebitigollawa and Medirigiriya. In 2011 cases were reported from Giribawa and Nikawewa, both in the North Western Province. A map drawn in 2013 showed that CKDu occurred most heavily in Siripura,-Padaviya-Medawachchiya-Horowopothana area, Medirigiriya-Polonnaruwa area, Dehiattakandiya- Girandurukotte area and the Nikawewa areas. It was therefore called Rajarata Kidney Disease.
REGISTERED CKDU PATIENTS UPTO DECEMBER 2014.
http://www.presidentialtaskforce.gov.lk/en/kidney.html#
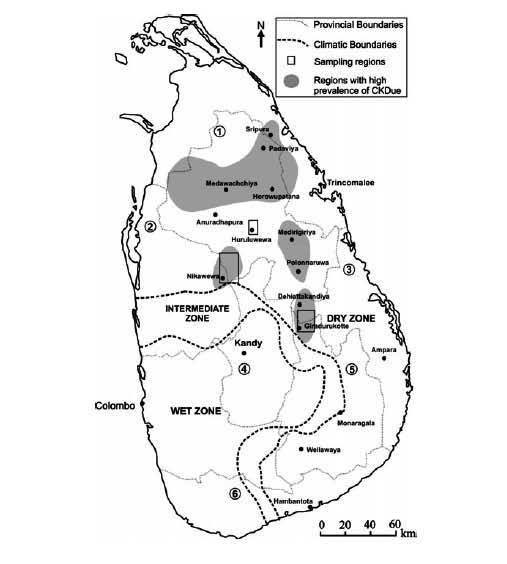
DISTRIBUTION OF CKDU
Source: H.R.A.L.N. Ranasinghe 2015 jas.sljol.info/articles/10.4038/jas.v10i2.8055/galley/6120/download
In 2015, the places with high prevalence of CKD/CKDu were Medawachchiya, Padaviya, Kebitigollawa, Rambawa, Medirigiriya, in the North Central Province (NCP), Wilgamuwa and Polpithigama in Kurunegala district , North Western Province, (NWP), Weli oya in Mullaitivu district, Northern Province (NP) , Siripura and Gomarankadawela, Trincomalee district, Dehiattakandiya , Ampara district, Eastern Province (EP) and Girandurukotte in Uva Province (UP). CKDU was thereafter found in Hambegamuwa in Uva province Angunakolapellassa and Bandagiriya in Hambantota district as well as Jaffna peninsula. New locations are emerging while the older locations continue to have the disease. CKDu is also reported from Egypt, El Salvador, Nicaragua and India’s Andhra Pradesh.
The numbers of CKDu patients, district wise from 2000 to 2013 were Anuradhapura 11,212 cases, Kurunegala 9781, Trincomalee 3858, Badulla 3141, Polonnaruwa 2957, Ampara 1118 and Batticaloa 325, making a total of 56,342 cases. WHO report 2012 stated that in the disease affected areas of the NCP at least 15% of people in the age group 15-70 years are affected by CKDu Ranjit Mulleriyawa observed that more than 8000 people were estimated to be receiving treatment in various parts of the country in 2013. Approximately 2600 patients are presently undergoing treatment at Girandurukotte hospital alone, he said.
In 2014-2015 the numbers were: Anuradhapura 3032, Polonnaruwa 6046, Badulla 3098, Vavuniya 1684 Kurunegala 1425 Matale 952 Ampara 671, Monaragala 587, Trincomalee 467, Mullaitivu 273 and Hambantota 312 making a total of 28576. (Source: National Health Strategic Master plan 2016-2025). Ministry of Health stated that in 2015 there were approximately 70,000 estimated CKD/CKDu patients in known high risk areas, the majority were from North Central Province. In 2016, Sri Lanka had the highest incidence of CKDu in South Asia, with around 180,000 people affected and approximately 50,000 deaths.
The cause (etiology) of this kidney disease is not known. Therefore the disease was named Chronic Kidney Disease of uncertain etiology” (CKDu). The features usually seen in kidney failure, such as diabetes, high blood pressure, obesity, snake bites or urinary tract infections were not seen in these kidney failure patients. The symptoms were also different. A study published in 2011, compared three rural populations in Medawachchiya, Yatinuwara (Central Province) and Hambantota (Southern Province). The known risk factors such as diabetes and hypertension were the main causes for CKD in Yatinuwara and Hambantota populations. These factors were absent in the Medawachchiya population.
A stream of research studies on CKDu were published from 2010 onwards. CKDu was attributed to various factors. These factors include hardness of drinking water, excessive amounts of fluoride in drinking water , presence of toxins produced by microorganisms such as cynobacteria in water, presence of the heavy metal cadmium in water, excessive use of fertilizers, insecticides, weedicides, contamination of water by agro-chemicals that contain high percentages of arsenic and mercury and combinations of these such as calcium content in hard water combined with arsenic in fertilizers and pesticides. Other possibilities considered were heat stress and excessive sweating, because NCP is the hottest area in Sri Lanka, use of low quality aluminum utensils for cooking and storing water and excessive consumption of poor quality, illegal liquor.
Despite the effort of about 60 researchers, including those funded by WHO, none of these hypotheses have been proved. Some assumptions were grossly inacceptable. High amounts of fluoride in the groundwater can be seen in all parts of the Dry zone while CKDu is highly prevalent only in a particular belt. Excessive use of fertilizers and agrochemicals such as glycophosphates can be seen in plenty in the wet zone, which is free of CKDu. In the Central Province, where agrochemicals are used at rates several times greater than the NCP, there is no CKDu. Aluminum utensils and poor quality illegal liquor are found all over the island. In one epidemiological study there seems to have been interference from the authorities to ‘the conclusions of the study.’
Since studies failed to find the cause for this CKDu and the etiology still remained largely unknown, WHO said in 2016 that exposure to a combination of factors that are toxic to the kidney, rather than one single factor, seems to cause this kidney disease. This illness is described, medically, as chronic kidney disease of unknown etiology, confined to certain geographical area in the country, with Irreversible damage to kidneys. No specific signs and symptoms, insidious onset which probably starts in second decade of life, slowly progressive and asymptomatic until very advanced. No cure in western system or any other system of medicine. The number of patients is increasing rapidly and it is becoming the biggest health issue in certain parts of the country. At the SLAAS theme seminar, December 2016, three speakers used ‘CKDu Sri Lanka’ in their lectures, one was a medical doctor, followed by a chemical engineer and sociologist . So CKDu, at long last, has come to the notice of the academic community. The conclusion is ‘this is a very serious problem that needs to be turned into a political issue.’
Almost all the CKDu patients in the North Central Province are Sinhala males, between 30 and 60 years, farmers engaged in rice cultivation. Farmers over the age of 40 years, who had been farming for more than 10 years, were at higher risk of developing the disease, said WHO. CKDu took 20-40 years to develop in a patient. The disease builds up stealthily in the body, manifesting only in advanced stages. It probably starts in the second decade of life. It is a slow progressive disease, where the kidneys reach the stage of irreversible damage, before the illness starts to show. By the time the victim realizes that there is something wrong with his health, the kidneys have been damaged beyond repair. Dialysis and transplants are the only treatments possible at this point. But patients tend to refuse dialysis because they found that those who failed to get dialysis regularly die faster. The patient invariably dies four years after they are diagnosed with the disease.
Ranjit Mulleriyawa observed that researchers failed to capture the depth of human suffering, the fear, anguish, desperation and trauma experienced by patients diagnosed with end state renal disease and their distraught families. Many suffer from mental health problems after they hear the diagnosis. Most continue to work till they die, they have no choice. When the father can no longer work, the entire family goes into financial ruin and debt. When he dies, the young wife and children are left desperate. Families become destitute, children get orphaned. The whole village gets impoverished. Individual families keep the illness secret, and till recently they did not know that many others in the same village were affected. ‘They never tell anyone’. ‘The young no longer want to work in the field, most have left the village and those who remain work in sand mining.
Bandarage noted that despite its emergence more than 20 years ago, the mystery surrounding the Rajarata Kidney Disease has not yet been solved. The scientific community ‘continues to be perplexed’ as to why CKDu is peculiar to the north central region and not the other rural areas of the country that have similar rice cultivation practices and lifestyles including extensive use of agrochemicals and aluminum utensils for cooking and storing water. The explanation may be political.
The North Central Province, (NCP) with its predominantly Sinhala population, lies between Northern and Eastern provinces, directly in the path of a merged North-east. The villages with the highest number of CKDu patients are adjacent to the Eelam boundary. Padaviya, Medawachchiya and Kebetigollawa lie in a belt along the Northern Province boundary. Siripura, Medirigiriya, Girandurukotte are close to the Eastern Province boundary. Most of these villages are in the ‘new areas’ opened by the Mahaweli scheme. `Kebetigollewa is in System L in the accelerated Maheweli scheme, Girandurukotte is in System C. Weli oya was created as a Sinhala settlement in 1984. Tamil separatists objected saying it was created to ‘delink the contiguity of Northern and Eastern Provinces’. Padaviya and Weli oya are among the ‘border villages’ brutally attacked by the LTTE. Therefore a charge of Genocide must be considered.

The Convention on the Prevention and Punishment of Genocide (1948) defines Genocide as ‘intent to destroy, in whole or in part, a national, ethnic, racial or religious group, by deliberately inflicting on the group conditions of life calculated to bring about its physical destruction. It is not necessary to destroy the entire group. Destruction of only part of a group is also genocide.’
Genocide could be achieved by the ‘deliberate release of harmful biological agents in order to cause death in people.’ These biological agents are altered to increase their ability to spread into the environment, to cause disease and make them resistant to current medicines. These agents can be spread through the air, water or food. They are extremely difficult to detect as they do not cause illness immediately.
The biological agent used in Sri Lanka, researchers deduce, must be made of chemicals having the following characteristics. It must be capable of forming stable complexes with hard water, capable of retaining nephrotoxic metals and delivering them to the kidney and capable of multiple routes of exposure, including ingestion. The agent has been introduced to the area in the last 20 to 30 years.
The evidence points to waterborne chemicals. Prof Oliver Illeperuma and CB Dissanayake reported a close association between CKDu and quality of drinking water. CKDU disease very likely occurs from the admission of harmful substance to the human body through water over an extended period of time, said the OPA Think Tank. WHO looked at the variables examined in the various studies, dismissed most of them and stated that only water should be given a research priority. Strengthen ongoing water quality surveillance, with a focus on nephrotoxic chemicals in the affected areas, WHO recommended.
In the North Central Province, the disease was found in areas where drinking water was drawn from the ground, particularly stagnant water from shallow wells and pipelines. It was more prevalent among those who drank water from wells situated below a reservoir or an irrigation canal. The disease was absent in areas where drinking water was obtained from natural springs and rivers. ‘Some unmeasured toxin’ in dug well water may have caused this, said SLAAS. Some doctors were more explicit. The well water is contaminated with toxic chemicals, they said.
CKDu has been identified by the medical profession from 1991, which means that it had started to take effect at least a decade before that. But there was no outcry about it . CKDu came to the attention of the authorities only twenty years later. Premini Amerasinghe made pointed reference to the deadly effect of CKDu in her novel Tangled threads’ ( 2010). The present government has produced a knee jerk solution. They have banned agro chemicals containing glycophosphates and advocated traditional rice varieties such as henati which have a poor yield. These decisions hit the farmers even more. They benefited by the new improved rice varieties like BG 360 which gave double the yield of the traditional varieties. So the remedy is no better than the disease.( Continued)
December 10th, 2016 at 6:33 pm
Unfortunately there is no racial profiling of CKDU affected persons. An analysis on these lines might shed some lights.
December 11th, 2016 at 9:49 pm
A good analysis. CKD didn’t occur naturally in these areas. It started only after heavy use of certain agrochemicals. Some large importers of these agrochemicals have political views sympathetic to separatists. These companies and international manufacturers have a huge clout on the matter. They are known to bribe people to defend them as this is a multibillion dollar industry.
December 18th, 2016 at 11:13 am
This is a valuable article. Thank you, Kamalika.
The LTTE attacked Lankans in any whichway possible to achieve Eelam.
The CKD through Glyphosate, in relation to the worst affected areas, can be linked to LTTE action. More studies ought to be done and the point proven and presented to the UN and other international bodies.
As the CKD started in those areas about 30 yrs ago, it all commenced during the Cold War period. Tamil Caste dissent which tied onto Cold War politics, continue to this day
The Trinco Port is also an important point in this connection.
December 18th, 2016 at 5:24 pm
Fran,
“The CKD through Glyphosate, in relation to the worst affected areas, can be linked to LTTE action.”
And who are the BIGGEST importers of GLYPHOSATE to SL?
Hint: Even after it was banned for good by Sirisena a certain Tamil large business imported CONTAINERLOADS of it. Guess what is was?
Now you see the connection!
Don’t forget these people are RICH. They have BOUGHT OVER some “PATRIOTIC” SL people!!
December 18th, 2016 at 5:29 pm
Kamalika,
There is NO CKDu.
It is CKD.
The “u” was introduced by some interested parties to whitewash the manufacturer.